Chronic Kidney Disease: Stages, Progression, and Early Detection
Most people don’t realize their kidneys are failing until it’s too late. That’s because chronic kidney disease (CKD) doesn’t scream for attention. No sharp pain. No fever. Just quiet, slow damage - often unnoticed until the organs are barely working. And yet, 37 million Americans have CKD, and 9 out of 10 don’t even know it. The good news? If caught early, progression can be slowed - even stopped. The key is understanding the stages, recognizing the warning signs, and knowing exactly when to act.
What Chronic Kidney Disease Really Means
CKD isn’t a single event. It’s a long, silent process where your kidneys lose their ability to filter waste, balance fluids, and make hormones that control blood pressure and red blood cell production. The official definition? Kidney damage lasting three months or longer. Damage doesn’t always mean scarring or tumors. It can be as simple as protein leaking into your urine - something your kidneys shouldn’t let through.
The system we use today was refined in 2012 by the Kidney Disease: Improving Global Outcomes (KDIGO) group. It’s not just about how well your kidneys filter blood. It’s about two things: how much blood they filter and how much protein leaks out. These are measured using two simple tests: a blood test for eGFR and a urine test for albumin-to-creatinine ratio (ACR). Together, they tell a full story.
The Six Stages of CKD: More Than Just Numbers
CKD is broken into five stages based on eGFR - estimated glomerular filtration rate. This number tells you how efficiently your kidneys are filtering waste from your blood. But here’s the catch: a low eGFR doesn’t always mean disease. And a normal eGFR doesn’t always mean your kidneys are safe.
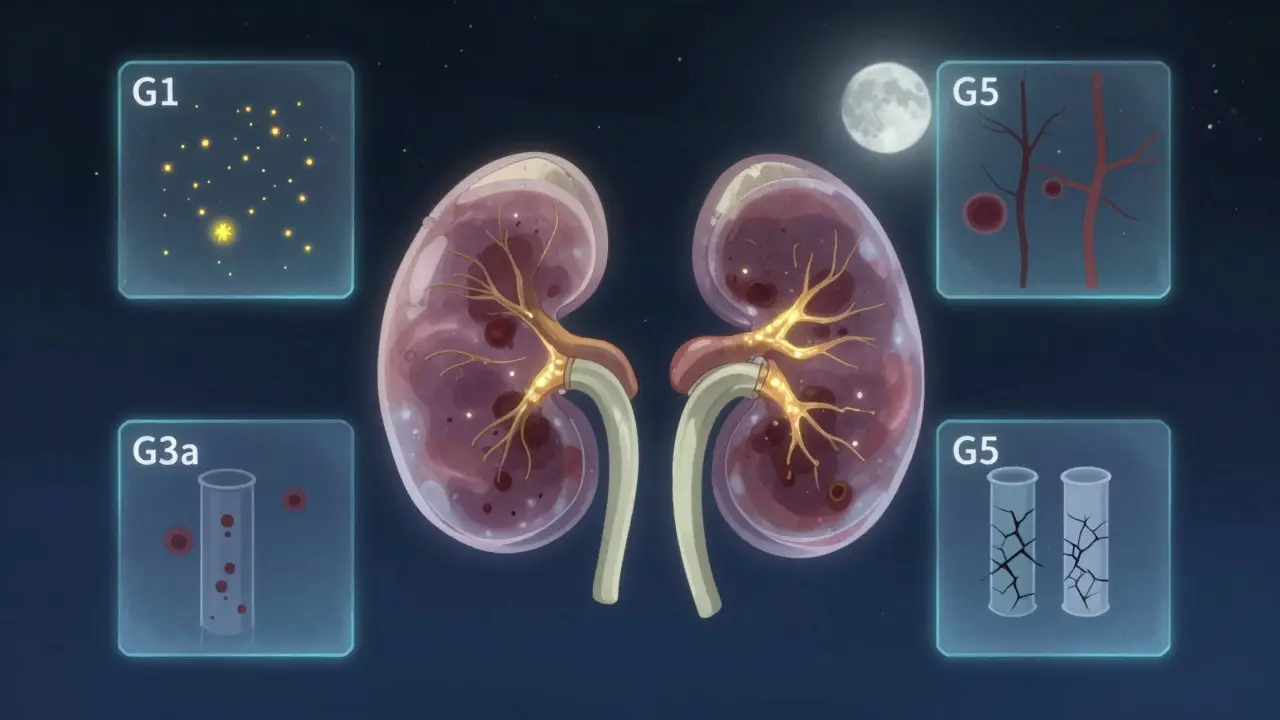
Stage G1: eGFR ≥90 mL/min/1.73m²
You might think this is healthy. And technically, yes - your kidneys are filtering at 90% or more of normal capacity. But if you have protein in your urine (ACR ≥30 mg/g), or structural damage seen on an ultrasound, or a history of kidney disease, you’re still in Stage G1. This is where CKD starts - quietly. No symptoms. No warning. Just a lab result that says, "Something’s off. Watch this."
Stage G2: eGFR 60-89 mL/min/1.73m²
Here, kidney function is mildly reduced. But again, if your urine test shows persistent protein leakage, you’re classified as CKD. Many people in this stage are diagnosed during routine blood work for unrelated issues - a high blood pressure check, a diabetes screening, or even before knee surgery. One nurse from Texas told her story: "I had ankle swelling I blamed on standing all day. My doctor found protein in my urine during a pre-op check. That’s when I learned I had CKD. I felt fine. I still do."
Stage G3a: eGFR 45-59 mL/min/1.73m²
This is the turning point. You’re now in the middle of the spectrum. Your kidneys are working at less than half their peak capacity. If you also have moderate to high albuminuria (ACR ≥30), your risk of progressing to kidney failure jumps. Studies show that patients in G3a with high protein levels have a 37% lower chance of advancing to G4 if they start ACE inhibitor medications. These drugs aren’t just for blood pressure - they protect the kidneys themselves.
Stage G3b: eGFR 30-44 mL/min/1.73m²
Now the risk spikes. People in G3b are 2.6 times more likely to reach kidney failure within five years than those in G3a. This is the stage where most doctors refer you to a nephrologist. If you’re diabetic, hypertensive, or have heart disease, this is non-negotiable. Delaying a specialist visit here can mean missing the window to slow damage.
Stage G4: eGFR 15-29 mL/min/1.73m²
Your kidneys are now working at less than 30% capacity. Symptoms may finally appear: fatigue, swelling in legs, nausea, trouble concentrating. But even now, it’s not too late to delay dialysis. Many patients who start preparing early - adjusting diet, managing blood pressure, controlling diabetes - can stay off dialysis for years. The key? You need a nephrologist. Not just a general doctor. And you need a plan.
Stage G5: eGFR <15 mL/min/1.73m² (or on dialysis)
This is kidney failure. Your body can’t clean itself anymore. You need dialysis or a transplant to survive. Ninety-eight percent of patients at this stage will eventually require one of these treatments. The goal of all earlier stages is to keep you from ever getting here.
Albuminuria: The Silent Red Flag
eGFR alone doesn’t tell the whole story. That’s why albuminuria matters just as much.
Albumin is a protein your kidneys normally keep in your blood. When they’re damaged, it leaks into your urine. The more that leaks, the worse the damage. ACR levels are grouped into three categories:
- A1: Less than 3 mg/mmol - normal to mildly increased
- A2: 3-30 mg/mmol - moderately increased
- A3: Over 30 mg/mmol - severely increased
Here’s the startling part: someone with A3 albuminuria - even with normal eGFR - has a 5.4 times higher risk of death than someone without it. That’s why doctors now combine eGFR and ACR into a single risk profile. A person with Stage G3a and A3 albuminuria is at far greater risk than someone with G3a and A1. This combo is what helps doctors decide who needs aggressive treatment and who can just be monitored.

Why Early Detection Saves Lives
Most people with CKD never feel sick - not until it’s too late. In fact, a 2022 survey by the National Kidney Foundation found that 78% of patients had no symptoms when diagnosed at Stage G2 or G3. They found out because of a routine blood test.
But here’s the power of catching it early: patients diagnosed before Stage G4 are 32% more likely to follow their treatment plan and 41% more confident in managing their health. Why? Because they had time. Time to learn. Time to adjust. Time to protect what’s left.
One man from Ohio, diagnosed at G3a after a diabetes check-up, changed his diet, started walking daily, and took his blood pressure meds without fail. Five years later, his eGFR is still at 52. He’s not on dialysis. He’s not even close.
But for others, the delay is deadly. A Reddit user shared: "I felt tired all the time. I thought it was stress. By the time I went to the doctor, my eGFR was 19. They said I should have been tested years ago. I was diabetic. They never checked my kidneys."
Who Should Be Tested - And When
You don’t need to wait for symptoms. If you have any of these, get tested every year:
- Diabetes (Type 1 or Type 2)
- High blood pressure
- Heart disease
- Obesity (BMI over 30)
- A family history of kidney failure
- Being African American, Native American, or Hispanic (higher risk groups)
- Age 60 or older
The test is simple: a blood draw for creatinine (to calculate eGFR) and a first-morning urine sample for ACR. No fasting needed. No needles. Just two quick tests. And they must be done twice, at least 90 days apart, to confirm CKD - because a one-time abnormal result could just be dehydration, infection, or medication side effects.
The Real Problem: Overdiagnosis and Underdiagnosis
There’s a debate in nephrology right now. On one side, doctors say we’re missing too many cases. On the other, they worry we’re labeling healthy older adults as sick.
Here’s the truth: 40% of adults over 70 have an eGFR below 60 - but their kidneys are aging, not failing. Their muscle mass is lower, so creatinine levels drop. Their filtration naturally slows. That’s normal. But if you just look at the number, you might call it CKD. That’s why experts now say: don’t diagnose CKD in older adults unless there’s also protein in the urine or clear signs of damage.
At the same time, we’re missing younger people. A 2023 study in Baltimore used mobile testing units and found 1,247 previously undiagnosed cases - 43% of them in Stage G1 or G2. These were people with no symptoms, no known risk factors. Just people who never got tested.
What’s Next: AI, Genetics, and the Future of Detection
The tools are getting smarter. In 2023, the FDA approved the first AI tool - AION nephro™ - that predicts kidney decline with 88.7% accuracy. It looks at 27 data points: blood pressure, glucose, cholesterol, age, meds, even how often you’ve been hospitalized. It doesn’t replace the doctor - it helps them see what humans might miss.
And soon, genetics will play a role. Researchers have identified 17 gene variants that strongly predict who will progress fastest. Within five years, a simple DNA test could tell you your personal risk - not just whether you have CKD, but how fast it might move.
For now, the best tool is still the one we’ve had for decades: regular testing. Especially if you’re at risk.
What You Can Do Today
You don’t need a specialist to start protecting your kidneys. Here’s what works:
- Control your blood sugar - if you’re diabetic, keep HbA1c below 7%
- Keep blood pressure under 130/80 - even if you don’t have high BP, this target helps your kidneys
- Reduce salt intake - less than 2,300 mg per day (about one teaspoon)
- Avoid NSAIDs like ibuprofen or naproxen long-term - they can damage kidneys
- Stay hydrated - water helps your kidneys flush toxins
- Ask your doctor for an eGFR and ACR test - don’t wait for symptoms
CKD isn’t a death sentence. It’s a warning. And like any warning, it’s only dangerous if you ignore it.
Can chronic kidney disease be reversed?
Early-stage CKD (Stages G1-G3a) can often be slowed or stabilized with lifestyle changes and medications like ACE inhibitors or SGLT2 inhibitors. But once significant scarring occurs - usually after Stage G3b - the damage is permanent. The goal isn’t reversal; it’s stopping further decline.
Do I need to see a kidney specialist if I’m in Stage G3?
If your eGFR is below 45 (Stage G3b) or if you have high albuminuria (ACR ≥30), yes - a nephrologist should be involved. Even in Stage G3a, if your eGFR is dropping fast (more than 5 mL/min/year) or you have diabetes or heart disease, a specialist can help tailor treatment to protect your kidneys.
Why do some people with low eGFR not have CKD?
In older adults, eGFR naturally declines due to reduced muscle mass and normal aging. Without protein in the urine or signs of structural damage, this isn’t considered true CKD. Doctors now avoid labeling these cases to prevent unnecessary stress and treatment.
Can I test for CKD at home?
You can’t fully test for CKD at home. Urine dipsticks can detect protein, but they’re not accurate enough for diagnosis. The gold standard is a lab test for albumin-to-creatinine ratio (ACR) and a blood test for creatinine to calculate eGFR. These require medical labs. Some pharmacies offer point-of-care eGFR tests, but they still need to be confirmed by a doctor.
Is CKD only a problem for people with diabetes or high blood pressure?
No. While diabetes and high blood pressure cause about two-thirds of cases, other causes include glomerulonephritis, polycystic kidney disease, long-term NSAID use, and even recurrent kidney infections. Anyone can develop CKD - which is why routine screening matters, even if you feel fine.
Lisandra Lautert
February 21, 2026 AT 13:17Cory L
February 22, 2026 AT 22:57Vanessa Drummond
February 23, 2026 AT 00:11Gabrielle Conroy
February 24, 2026 AT 22:15John Smith
February 26, 2026 AT 22:08Bhaskar Anand
February 27, 2026 AT 21:46Joanna Reyes
February 28, 2026 AT 18:12Christopher Wiedenhaupt
March 1, 2026 AT 10:48Christopher Brown
March 3, 2026 AT 05:19Sanjaykumar Rabari
March 5, 2026 AT 03:10